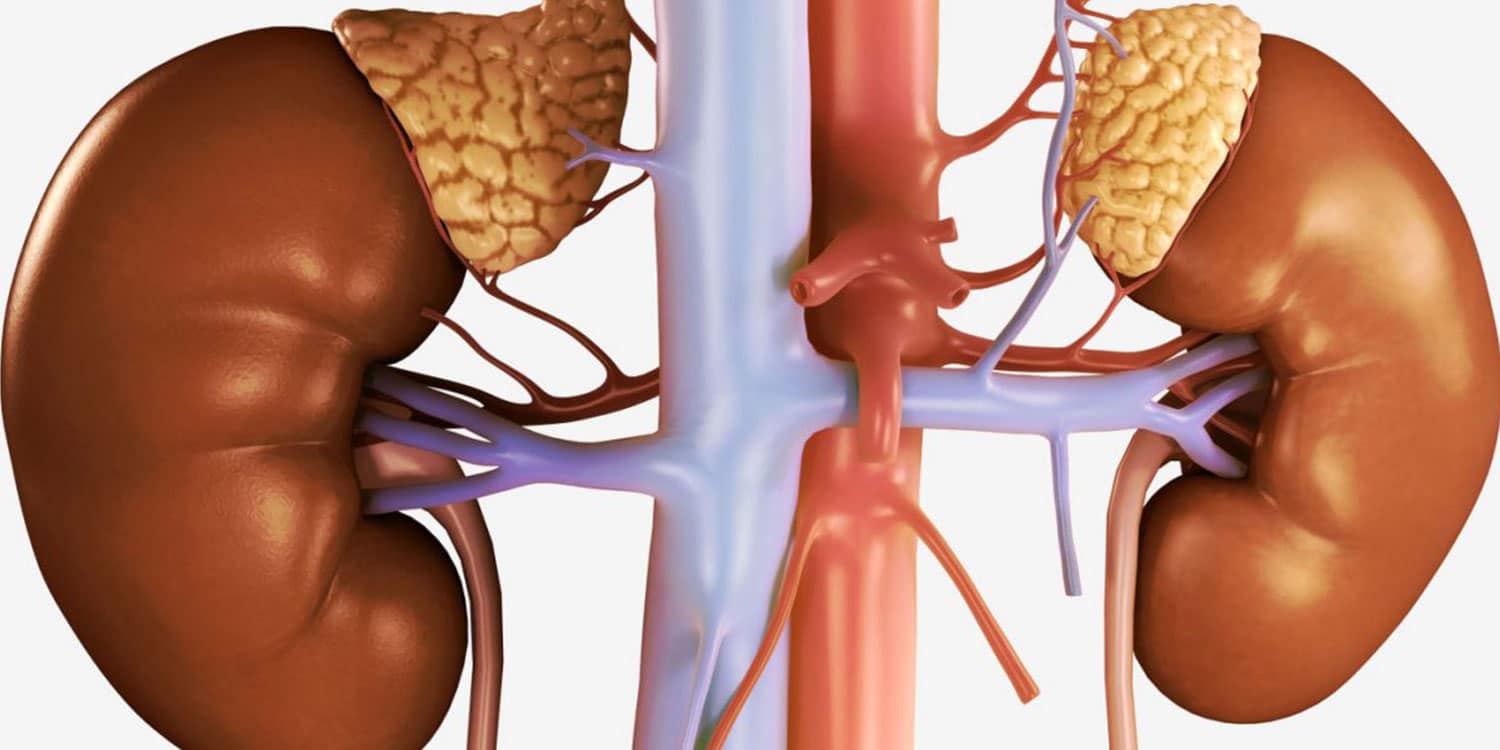
Adrenal disorders are due to the excessive or extremely small production of a specific hormone. The adrenal glands, which are located just above each kidney, consist of two layers: the cortex and the medulla. They are responsible for the production of hormones that help the body control blood glucose levels, metabolise proteins and fat, regulate blood pressure and suppress the inflammatory response of the immune system. The most important hormones produced in the cortex are cortisol, aldosterone and androgens, while the medulla produces adrenaline.
Adrenal disorders: Cushing’s Syndrome
Cushing’s Syndrome is caused by excessive production or use of cortisol. It occurs at a frequency of 1:1000000 and is either exogenous or endogenous.
Exogenous Cushing’s Syndrome: Results from the intake of medication called glucocorticoids that mimic cortisol. These pharmaceutical formulations are used to treat asthma or rheumatoid arthritis, and systemic lupus erythematous, for long periods and in high doses.
Endogenous Cushing’s Syndrome: Results from excessive cortisol production by the adrenal glands due to problems:
- In the pituitary gland: benign tumours that suppress the hormone. This is the most common form of Cushing’s Syndrome.
- In the adrenal glands: benign and (rarely) malignant tumours or bilateral nodular adrenal hyperplasia. It is known as Cushing’s Adrenal Syndrome and is found in only a small percentage of patients.
- In non-pituitary or non-adrenal tumours: this very rare form is known as Cushing’s Syndrome due to ectopic hyper-secretion of cortisol.
Adrenal Disorders: Symptoms of Cushing’s Syndrome
The symptoms of Cushing’s Syndrome develop gradually and worsen if the condition is not diagnosed early, depending on the cause of the syndrome, the degree of hyper-secretion, age and the levels of adrenal hormones.
- The most common symptom is weight gain, characterised by fat deposits in the facial area (moon face), throat and abdomen, while limbs are thin and weak.
- Skin is more sensitive, bruises easily and is at risk of infection.
- Wounds heal slowly and exhibit wide purple streaks.
- In girls with Cushing’s Syndrome, hyper-secretion of androgens leads to increased hair growth and menstrual disorders.
- Hyper-secretion of cortisol (hypercortolism) may cause blood glucose levels to increase, resulting in mellitus diabetes.
Adrenal Disorders: Diagnosis of Cushing’s Syndrome
The disease is diagnosed by an endocrinologist through a blood test measuring cortisol levels, a dexamethasone suppression test and CT or MRI imaging scans.
Adrenal Disorders: Treatment for Cushing’s Syndrome
The best treatment for Cushing’s Syndrome is to surgically remove the pituitary adenoma. If the disease persists, pituitary irradiation and adrenalectomy may be performed. Medication can also administered to inhibit the production of cortisol.
Adrenal Disorders: Adrenal Insufficiency
Adrenal insufficiency, also known as Addison’s Disease, is caused by the inability of the adrenal glands to produce sufficient cortisol and aldosterone. It has a primary and secondary form and is due to:
- Autoimmune disorders that damage adrenal glands.
- Infections such as tuberculosis or fungal infections.
- Non-activation of the adrenal glands by the pituitary gland and long-term administration of corticosteroids.
Adrenal Disorders: Symptoms of Adrenal Insufficiency
Symptoms of adrenal insufficiency depend on the rate of adrenal damage and the severity of the condition. They present in stages and the main symptoms include:
- Easy fatigue
- Anorexia
- Weight loss
- Weakness
- Dizziness
- Hyperpigmentation
- Hypoglycaemia
Adrenal Disorders: Diagnosis of Adrenal Insufficiency
The doctor takes a detailed history, conducts a clinical examination and orders lab tests to measure the levels of glucose, Na+ and K+, urine test, cortisol levels and ACTH, adrenal antibodies and stimulation test.
Adrenal Disorders: Treatment of Adrenal Insufficiency
Treatment, which is administered orally and for life, aims to replenish the missing hormones. The dose is adjusted to meet the needs of the patient (level of stress and age). The child should be monitored by an endocrinologist.
Adrenal Disorders: Congenital Adrenal Hyperplasia (CAH)
Congenital Adrenal Hyperplasia is a hereditary disorder characterised by the absence or insufficiency of the enzymes that produce adrenal hormones. In most cases the adrenal glands do not produce cortisol. The main enzyme is called 21-hydroxylase and is inherited in an autosomal recessive pattern, common in Mediterranean nationalities.
There are two types of CAH:
- Classic: the most serious form of the disease. Emerges in early childhood.
- Non-classic: a milder form that usually develops in late childhood.
Adrenal Disorders: Symptoms of Congenital Adrenal Hyperplasia
Symptoms in infants include:
- Ambiguous external genitalia in female new-borns (not typically female in appearance)
- Enlarged penis in boys
- Difficulty to gain weight
- Vomiting
- Irregular electrolyte levels.
Symptoms of CAH in older children:
- Early puberty
- Rapid growth
- Menstrual disorders in girls.
Non-classic CAH symptoms are usually more noticeable in young girls and include:
- Irregular or absence of menstruation
- Male characteristics, excessive body hair
- Deepening of the voice
In both sexes it provokes:
- Early puberty
- Rapid growth
- Acne
- Low bone density
- High blood cholesterol levels
Adrenal Disorders: Diagnosis of Congenital Adrenal Hyperplasia
The endocrinologist will evaluate the child’s symptoms and perform a clinical examination, followed by a series of blood and urine tests to measure cortisol, aldosterone and androgen levels, as well as a SYNACTHEN stimulation test.
Adrenal Disorders: Treatment of Congenital Adrenal Hyperplasia
Treatment depends on the form of the disorder. In classic CAH, it involves the administration of cortisol. The endocrinologist regularly monitors the child and the dose varies with age and stress levels. Non-classic CAH does not require hormone replacement therapy, although it may be required in puberty.
Infants with ambiguous genitalia may require surgery.
The Paediatric-Adolescent Diabetes clinic at MITERA Children’s Hospital is run by Dr Nikolaos Kefalas, Paediatrician-Endocrinologist. The team is comprised of nurses, paediatric endocrinologist, psychologist and clinical dietician-nutritionist who oversee the treatment, support and education of children with Type 1 and Type 2 diabetes, at both the initial diagnosis and during the subsequent progression of the disease.